Proton Therapy
The following are descriptions of several proton therapy research projects that our medical physicists are currently pursuing:
Single Energy Bragg Peak (SEBP) Delivery Technique
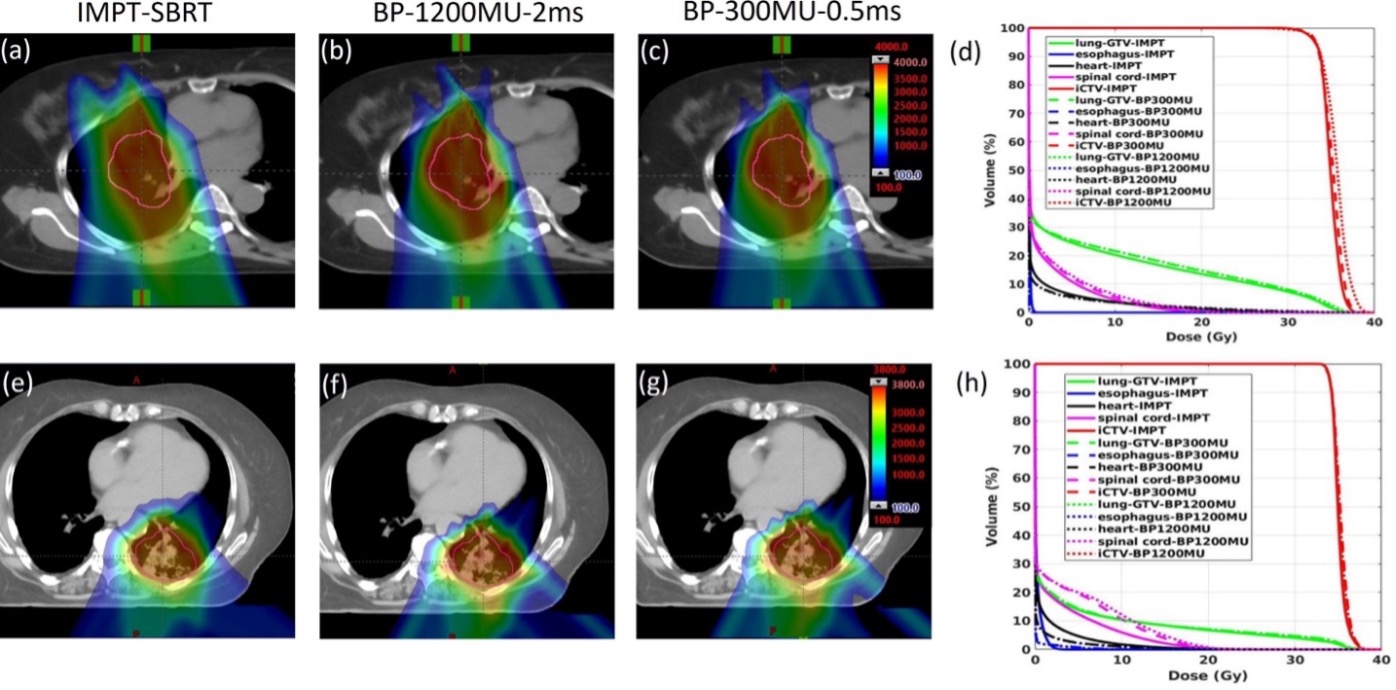
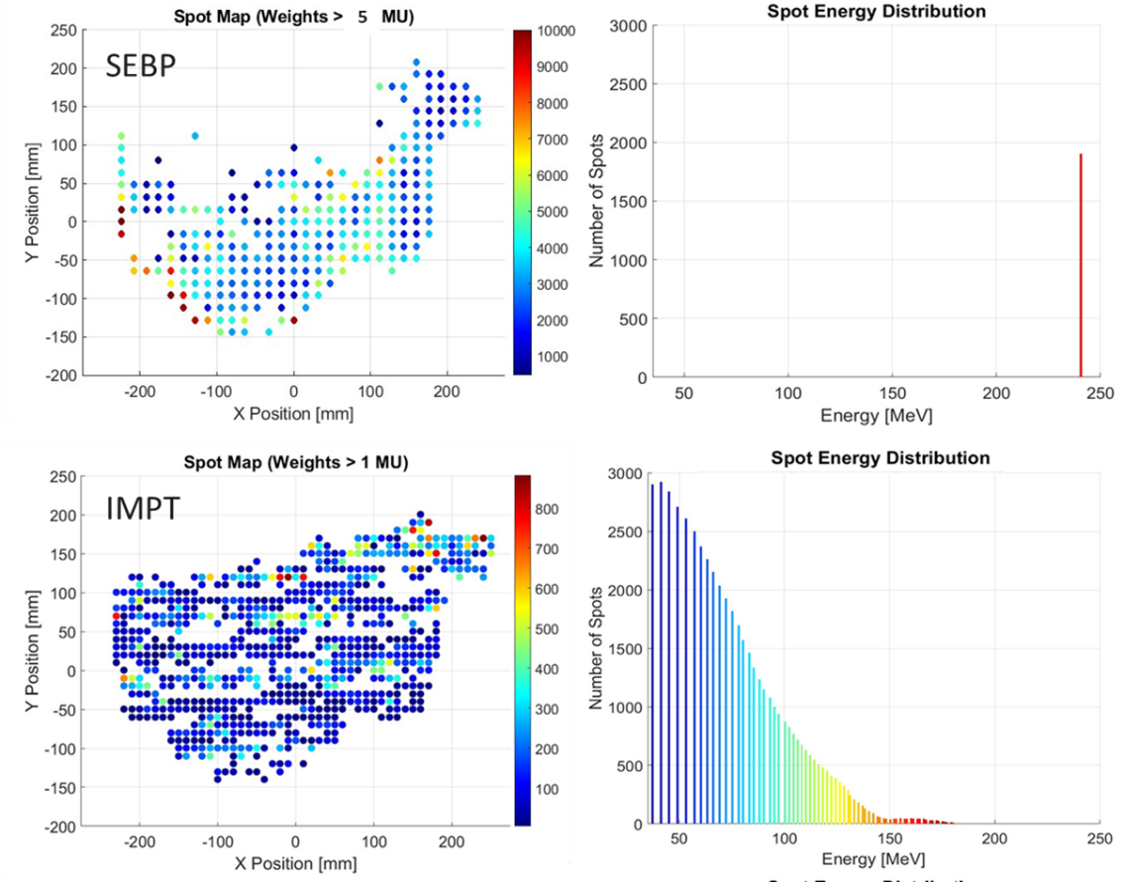
A major area of ongoing research within our group is the development and clinical translation of Single-Energy Bragg Peak (SEBP) proton therapy. SEBP is a novel treatment approach that uses a single high-energy proton layer combined with universal range shifters and patient-specific range compensators to position the Bragg peak at the distal edge of the target volume (Figure 1). By replacing the many energy layers required in conventional intensity-modulated proton therapy (IMPT), SEBP substantially simplifies treatment delivery while maintaining highly conformal dose distributions and the fundamental dosimetric advantages of proton therapy.
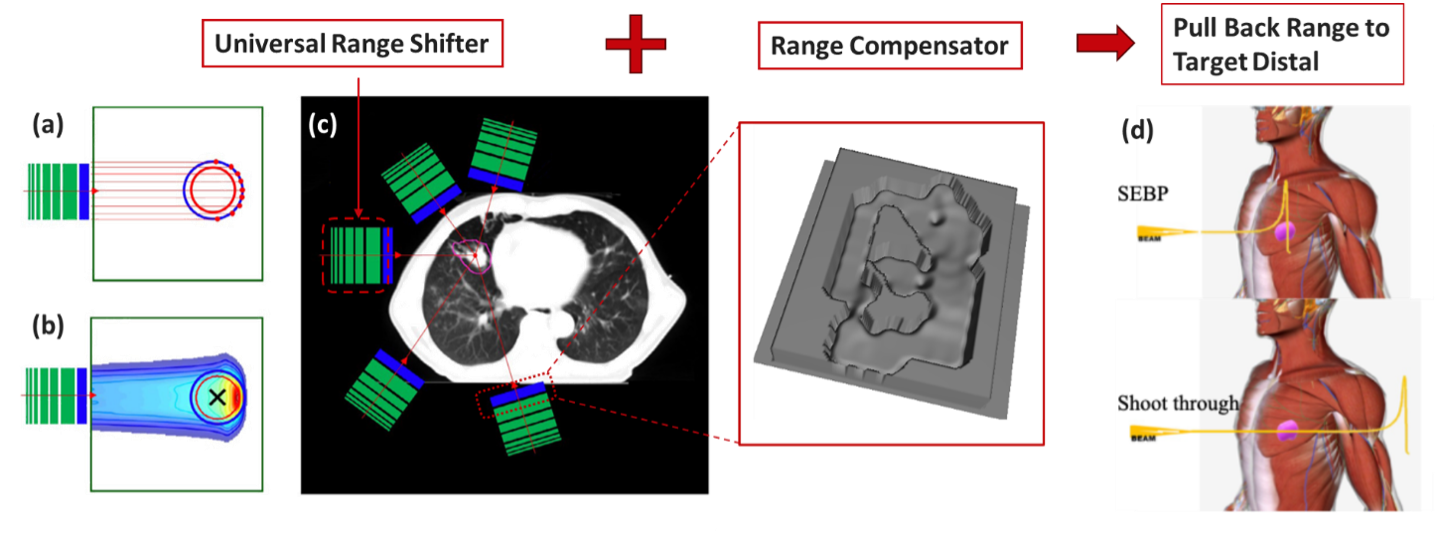
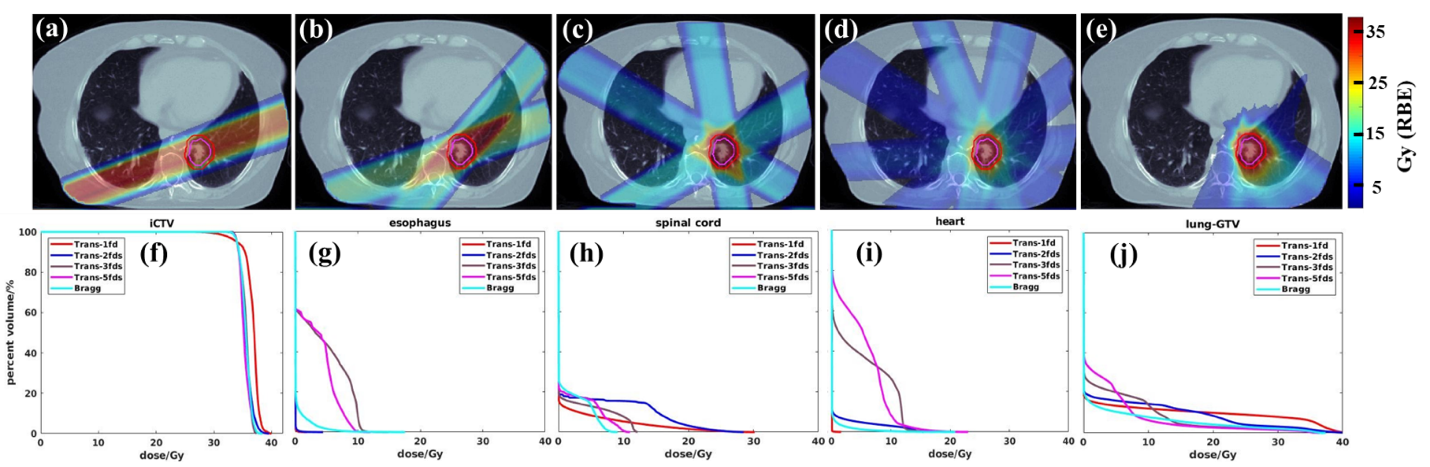
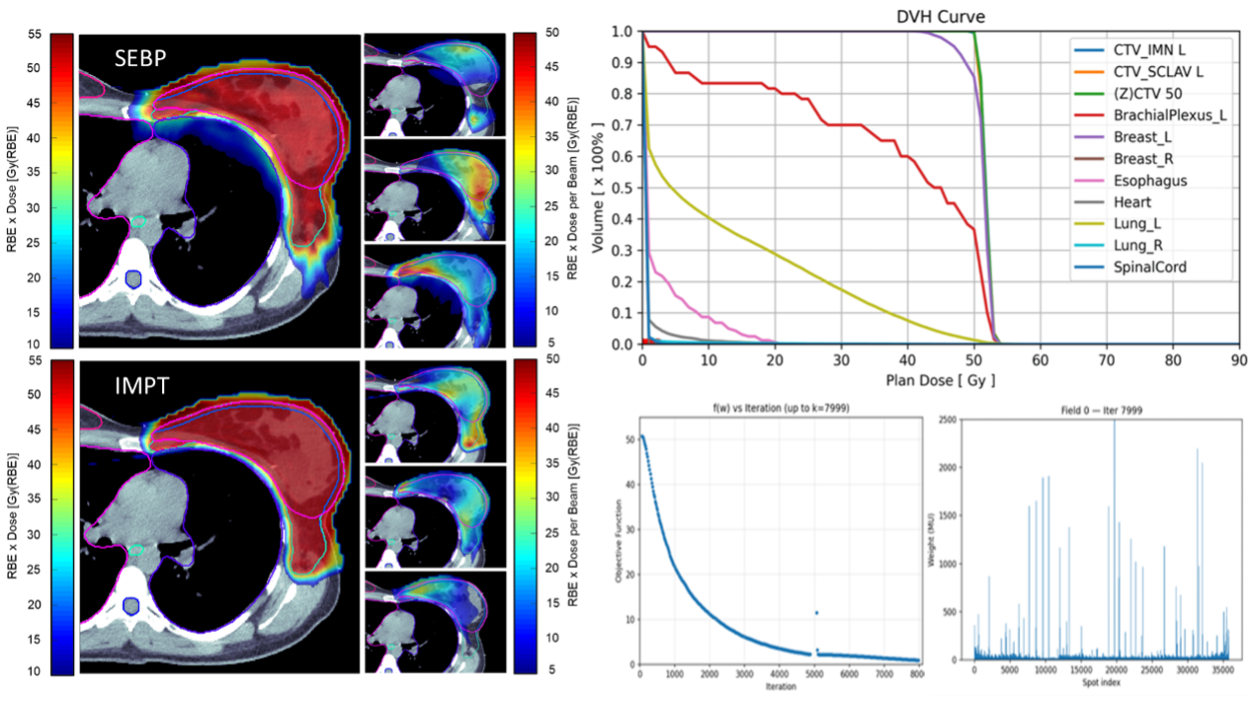
Unlike transmission proton FLASH, which relies on the entrance (plateau) region of the proton beam, SEBP FLASH utilizes the pristine Bragg peak to deliver conformal dose distributions (Figure 2). This approach has the potential to improve normal tissue sparing, reduce or eliminate exit dose, and expand the clinical feasibility of FLASH radiotherapy on existing proton therapy systems. Through inverse treatment planning and advanced optimization techniques, SEBP can achieve highly conformal dose distributions comparable to conventional multi-energy IMPT while substantially reducing delivery complexity (Figure 3). Current research efforts are evaluating SEBP for lung, liver, breast, pancreas, brain, and head & neck treatment sites.
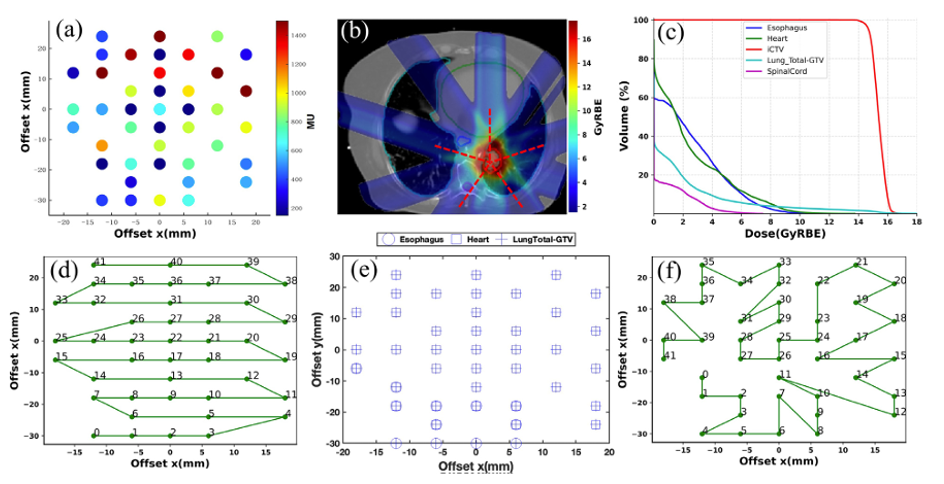
FLASH Dose Rate Optimization
Pencil beam scanning delivery speed depends on spot placement, delivery sequence, and the total number of spots. Our group is investigating dose rate optimization through intelligent spot sequencing, where delivery order is optimized using advanced algorithms to maximize ultrahigh dose rate coverage of critical organs at risk without altering the prescribed dose distribution or compromising conventional dosimetric metrics (Figure 4). These methods are being evaluated in phantom studies using realistic patient treatment plans, including both transmission and Bragg peak FLASH delivery techniques, with the goal of enabling practical and clinically implementable proton FLASH radiotherapy.
Sparse Spot Optimization for Moving Targets
Organ motion remains one of the major challenges in proton therapy, particularly for thoracic and abdominal treatment sites. Sparse spot optimization is a novel treatment planning approach that simultaneously optimizes proton spot intensities and spot positions, allowing treatment plans to be delivered using substantially fewer spots than conventional IMPT. Unlike traditional approaches that rely on a fixed spot grid, sparse spot optimization adaptively redistributes proton spots to maintain dosimetric quality while improving delivery efficiency (Figure 5).
When combined with motion management strategies such as deep inspiration breath hold (DIBH), this technique has the potential to reduce interplay effects and enable proton treatments to be delivered within a single breath hold. Preliminary studies have demonstrated substantial reductions in spot count, energy-layer complexity, and beam delivery time while maintaining clinically acceptable dosimetry. Current investigations include breast and liver proton therapy, with a focus on plan quality, robustness, and treatment efficiency (Figure 6).
Range Uncertainty Reduction
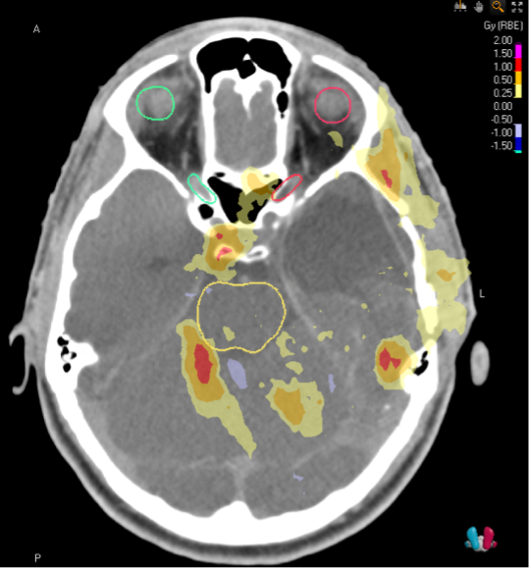
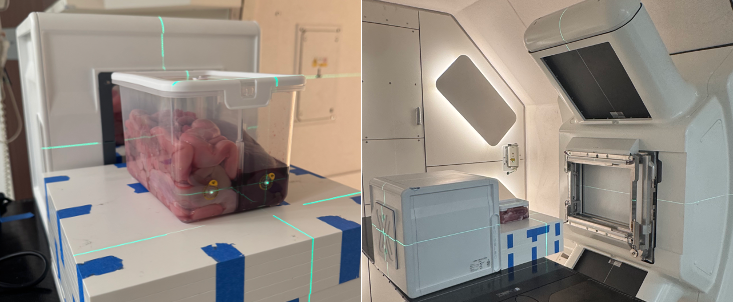
The typical clinically acceptable range uncertainty for proton planning is 3.5%; however, studies have found that through the use of dual energy computed tomography (DECT) this can be reduced to 2% due to improved stopping power ratio (SPR) calculation accuracy. By acquiring images at two distinct x-ray energies, DECT enables more accurate material characterization, which improves SPR calculations. Our group is investigating the application of DECT based SPR calculations in proton treatment planning where the reduced range uncertainty results in lower doses to the surrounding tissue (example in Figure 6). This work also includes the validation of DECT derived SPR calculations using animal tissues and advanced detection systems (Figure 7).
Commissioning and Clinical Implementation
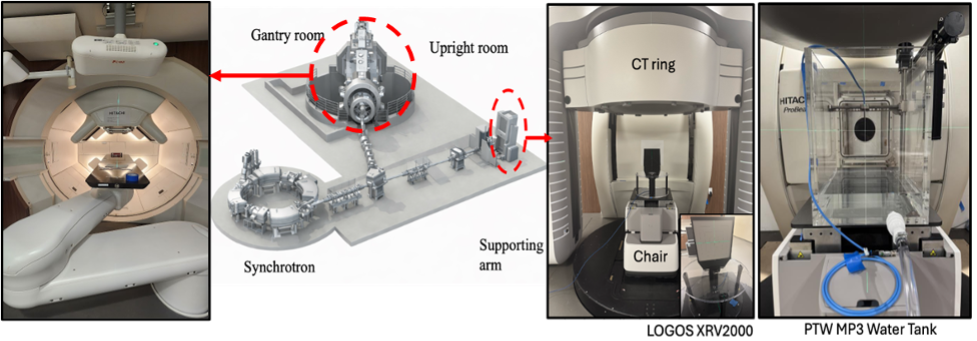
A major focus of our current work is the commissioning and clinical implementation of the new proton therapy program at the University of Wisconsin. The facility is based on a Hitachi ProBeat proton therapy system and includes both a rotating gantry treatment room and a novel upright fixed-beam treatment room (Figure 9). The upright treatment platform incorporates a Leo Cancer Care chair with six-degree-of-freedom (6D) patient positioning and a vertical CT imaging system, enabling simulation, image guidance, and treatment delivery in the upright position. Ongoing efforts include beam characterization, treatment planning system commissioning, image guidance validation, motion management, end-to-end testing, and the development of clinical quality assurance workflows.
In parallel, we are investigating novel proton dosimetry and QA technologies, including a combination strip/multilayer ionization chamber system and scintillation based detectors for beam characterization, spot verification, range measurements, and treatment delivery validation. These efforts aim to improve the accuracy and efficiency of proton therapy commissioning and routine clinical quality assurance.
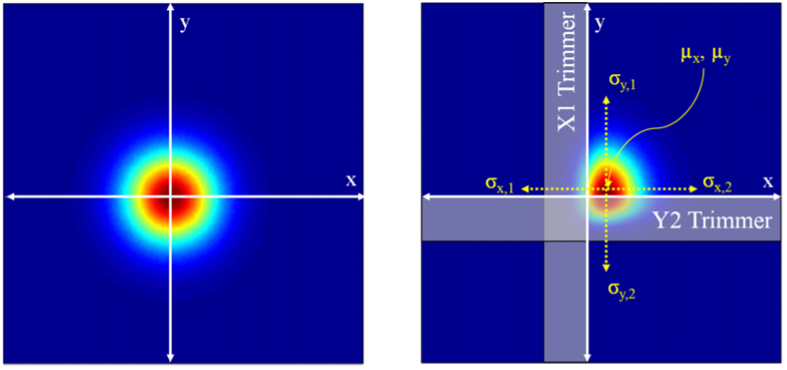
Penumbra Sharpening for Improved Dosimetry
Researchers in the Department of Radiation Medicine collaborate with others in the Department of Medical Physics, the University of Wisconsin Medical Radiation Research Center, and several other institutions across the country on a novel dynamic collimation system capable of “trimming” proton spots to sharpen dose falloff outside a treatment target. This device is specifically designed to maintain high dose to treatment targets while reducing dose and related toxicities in nearby normal tissues. Over many years the team has taken this from a theoretical concept to a working prototype integrated with the proton delivery system. Ongoing research efforts focus on the application of Monte Carlo and other modeling simulations to inform design choices, optimize delivery time and plan efficiency, and ensure robustness of the treatment execution.