Theranostics and Radiopharmaceutical Therapy
The following are descriptions of several theranostics and radiopharmaceutical therapy research projects that our medical physicists are currently pursuing:
Tumor Segmentation for RPT Dosimetry
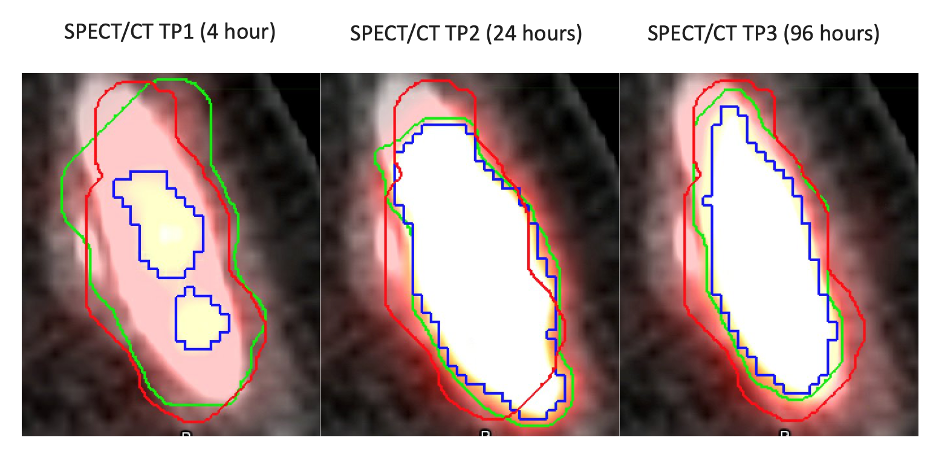
Radiopharmaceutical therapy (RPT) represents a rapidly advancing approach in oncology, enabling the delivery of targeted radiation to malignant tissues. Despite its promise, variability in tumor segmentation methods across institutions introduces significant uncertainty in dosimetric calculations, which may ultimately influence clinical decisions. In this work, we systematically evaluate the sensitivity of dose estimates to a range of segmentation techniques applied at multiple timepoints post-administration. Based on these analyses, we seek to define a standardized and reproducible tumor segmentation framework that can serve as a gold standard for RPT dosimetry.
Population Based Pharmacokinetic Modeling for Tumors and Normal Tissues
Personalized dosimetry in radiopharmaceutical therapy is essential for maximizing tumor control while minimizing normal-tissue toxicity. However, a critical—and historically variable—step in calculating absorbed dose is the pharmacokinetic (PK) fitting of time-activity curves. Currently, the lack of consensus on how these fits should be applied to individual organs and tumors introduces significant uncertainty into treatment planning. The motivation of this work is to address this variability by evaluating the impact of standardized PK fitting models on organ-specific dose estimates.
This research investigates whether a consensus or “most common” fitting method exists for distinct organs across clinical practices. To test this, the study compares best fitting curve approaches against an organ-specific, most common fitting method applied uniformly across a patient cohort. Ultimately, this work aims to quantify how the choice of PK model affects the final absorbed dose and to determine if adopting a standardized fitting strategy per organ can improve the consistency and reliability of future clinical dosimetry decisions.
Development of a Dosimetric Validation Framework for Clinical RPT Planning Systems
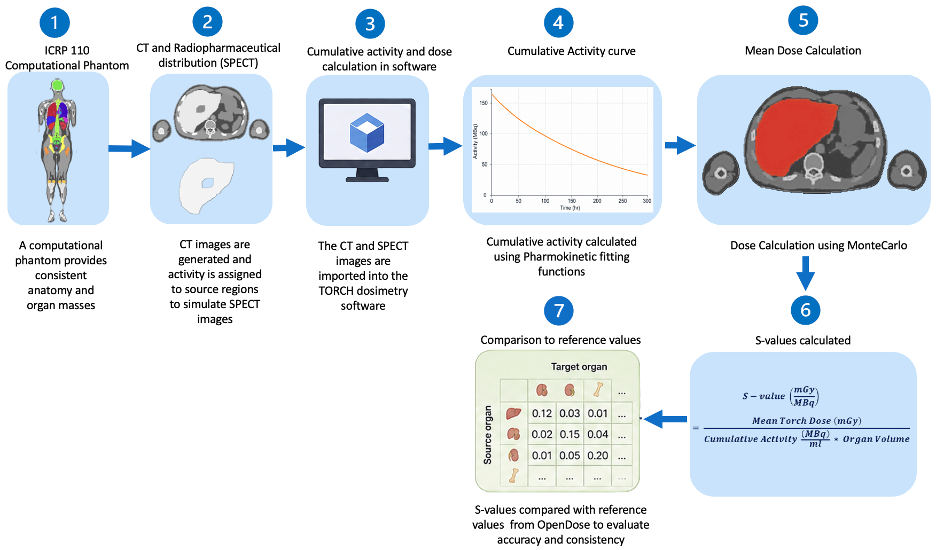
This project focuses on benchmarking radiopharmaceutical dosimetry planning systems using realistic computational human phantoms. It provides a framework to evaluate how different systems calculate and report radiation dose to organs and tissues following radiopharmaceutical therapy. By comparing dose estimates using standardized phantom-based data, the project helps improve the accuracy, consistency, and reliability of dosimetry tools, supporting safer and more confident treatment planning.
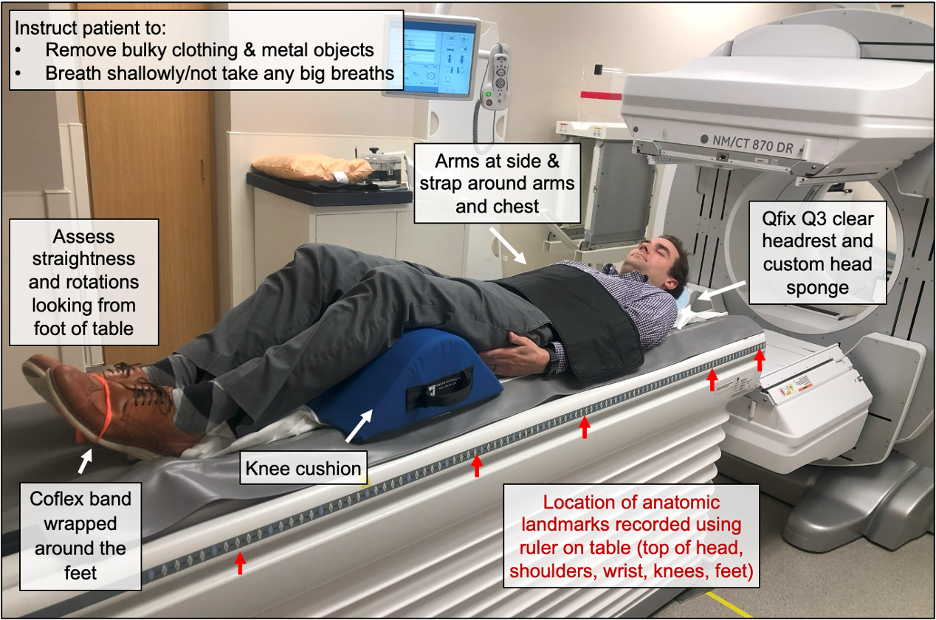
Standardized immobilization and setup procedure for multi-time point SPECT/CT image registration for RPT dosimetry
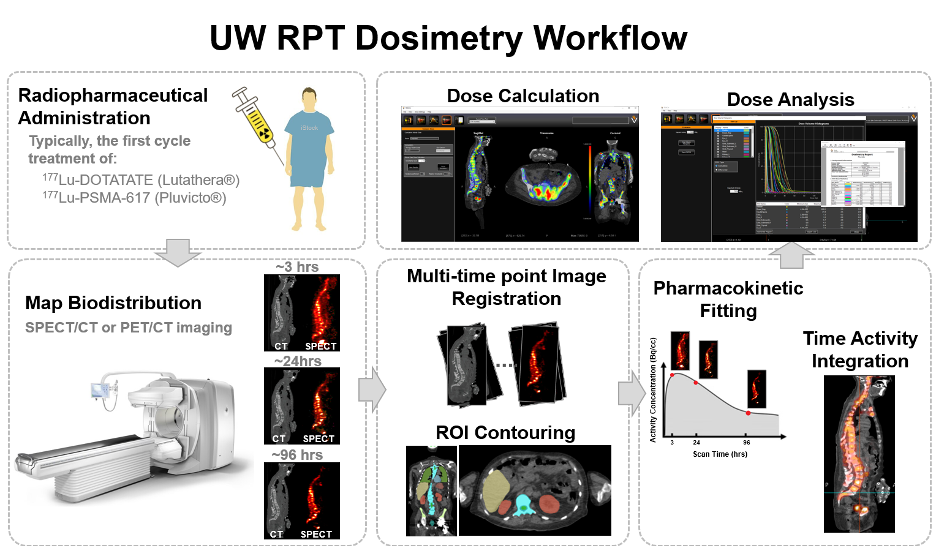
In order to perform voxelized radiopharmaceutical therapy (RPT) dosimetry, patients are imaged using SPECT/CT at several time points after their first cycle of 177Lu-PSMA-617 (Plucvito) or 177Lu-DOTATATE (Lutathera). Since small differences in patient positioning can make image registration between the different scans challenging, we developed a simple standardized immobilization and setup procedure for patients undergoing SPECT/CT imaging. This was shown to significantly improve deformable image registration accuracy, helping reduce dosimetric uncertainties and supporting more reliable personalized RPT treatment planning.
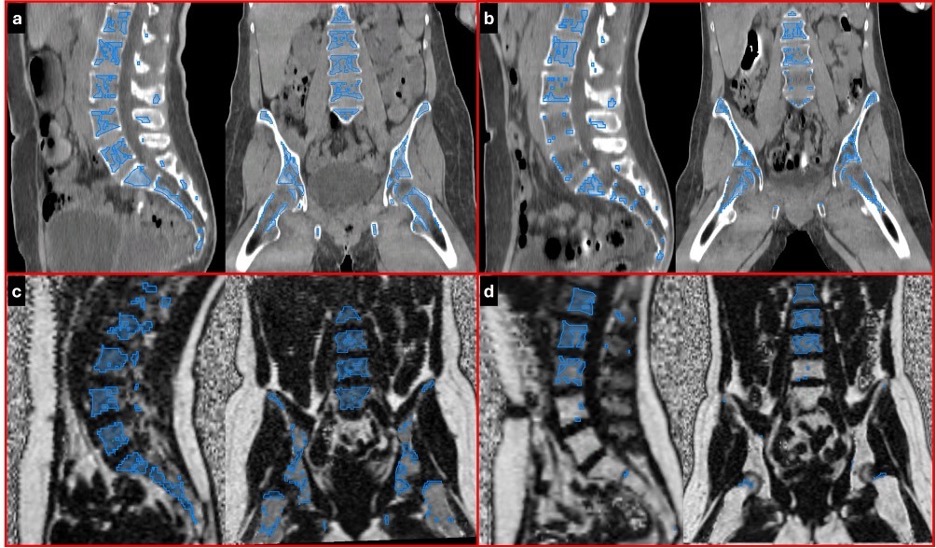
Deformable Image Registration for Theranostics
Deformable image registration (DIR) plays a critical role in theranostics where accurate alignment of multimodality and multi-timepoint imaging is essential for treatment planning, response assessment, and patient-specific dosimetry. In the RPT workflow, imaging is acquired across different modalities and at multiple time points, with anatomical changes occurring between scans. DIR enables mapping of structures across these datasets, supporting voxel-based dose accumulation and improved estimation of dose. However, uncertainties in DIR accuracy, particularly in the presence of anatomical deformation and low-contrast functional imaging, remains a challenge and are difficult to quantify in patient data due to lack of ground truth.
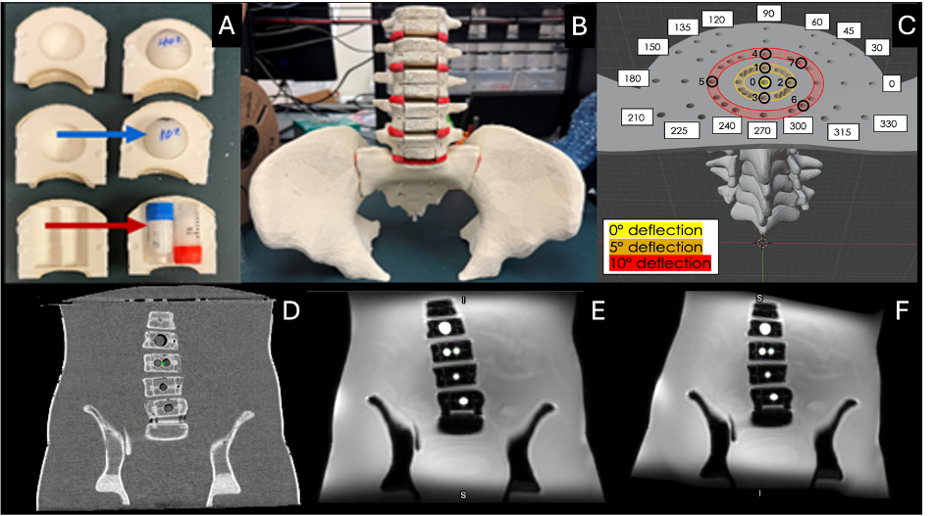
To address this, we have developed a novel 3D-printed anthropomorphic DIR phantom designed to support validation of multimodality imaging and quantitative workflows in theranostics. The phantom incorporates anatomically realistic lumbar spine and pelvic structures and enables controlled, reproducible deformations with known ground truth, providing a unique framework for systematic evaluation of DIR performance. The phantom supports CT, MRI, and SPECT imaging and includes activity-filled inserts enabling lesion quantification and multi-timepoint imaging scenarios that closely mimic our clinical workflow.
Active Bone Marrow Dosimetry
Active bone marrow (ABM) is a critical organ in both radiation therapy and radiopharmaceutical therapy where it plays a central role in hematopoiesis and often represents a primary dose-limiting structure. Irradiation of ABM can lead to hematologic toxicity (HT), treatment delays, and reduced therapeutic effectiveness. A key challenge in modern therapy is that ABM is not evenly distributed throughout the skeleton both spatially and biologically. Current clinical approaches to assess marrow function are either invasive (biopsy) or not widely available such as F-18 Fluorothymidine Positron Emission Tomography (FLT PET).
Our research focuses on developing clinically accessible, non-invasive imaging approaches to identify and quantify ABM using fat fraction MRI (FFMRI) and multi-energy CT (MECT). In preclinical swine studies, we demonstrated that FFMRI provides strong agreement with gold-standard FLT PET for identifying proliferative marrow, while MECT offers a complementary modality for assessing marrow composition. In prospective human studies, we further showed that ABM is highly sensitive to radiation, with substantial reductions in ABM volume following therapy and clear dose-dependent changes in marrow composition. These findings support the integration of ABM imaging into treatment planning workflows, with the goal of enabling marrow-sparing radiation therapy and improving patient-specific dosimetry. Together, this work advances the development of biologically guided treatment strategies that aim to reduce toxicity while maintaining effective cancer control.